
- It is genetic defect confined to red blood cells. (RBCs) Transformation of biconcave shaped RBCs to Sickle like form is known as sickling process. Due to sickling there is early destruction of RBCs leading to condition like anaemia and is known as sickle cell anaemia. Scientists found that this phenomenon is due to defective haemoglobin inside the RBCs, hence the Haemoglobin inside the RBCs is known as Sickle cell haemoglobin
- Anaemia, mild jaundice and severe joint pain are major symptoms of the disease. Enlargement of spleen is found in majority of the patients. Due to repetition of sickling process in oxygen deficient condition, the sickle red cells entangle in each other and obstruct the blood flow in some part of the body, producing ischemia and tremendous pain. If prompt and proper treatment is not provided patient is likely succumb to death (sickle cell crisis). Such crisis episode usually occurs 2 to 4 times a year.
- This disease being hereditary in nature cannot be cured by medicine. Due to this chronic and incurable condition, patients along with their parents remain frustrated and vulnerable.
- Sickle cell anaemia is a genetic defect with autosomal recessive manner transfer of genes and hence found in two forms that is Heterozygote (AS) and Homozygote (SS) condition. Heterozygous individual commonly known as Carrier and homozygous individual as Sufferer. Carriers generally do not have any symptoms of disease but sufferer always suffers from various complications. When two individuals either carrier or sufferer or one carrier and another sufferer have a chance to have sufferer baby
Prevalence:
- The disease is found all over world, but common in Africa, Europe, Saudi Arabia and India. In India this disease or mostly found in alarming frequency in central part of India. This disease in India mostly found amongst scheduled caste (SC), scheduled tribes (ST) and Other Backward Communities (OBC). Hence it is also known as poor mans disease. Prevalence rate ranges from 0 to 40%.
Diagnosis:
- Since this is red blood cell disorder hence diagnosis is possible by performing few laboratory tests on blood sample. These tests are Solubility test and Electrophoresis test at alkaline pH. We at Maharashtra Arogya Mandal modified existing technology made it easy to implement on large scale. This modified test requires minimum blood quantity (3 to 4 drops by finger prick method) and is very cost effective. Since there is no continuous electric supply in remote tribal areas, we modified our equipment which will run on battery cells. This modification made it easy to work in isolated tribal areas
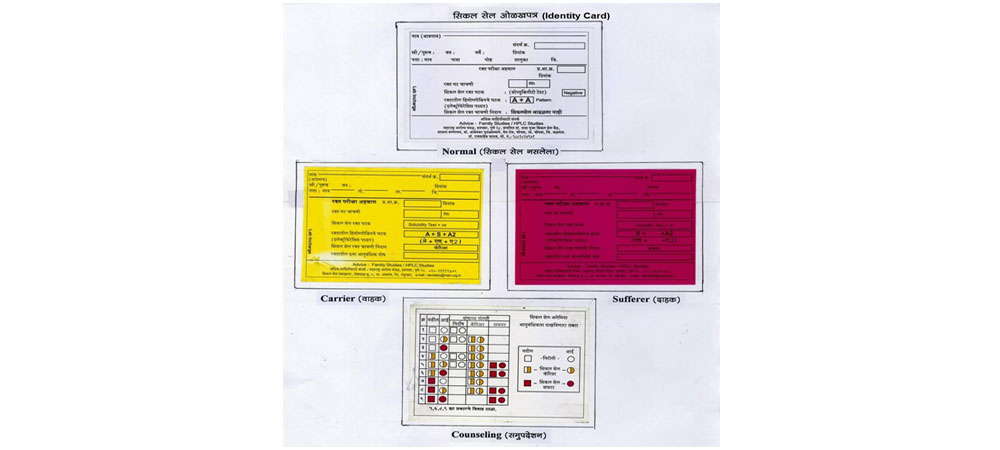
- By performing these two tests on blood sample, it is possible to identify carrier, sufferer and normal individual (without sickle cell defect)
| Solubility test | Electrophoresis band | Sickle cell status |
|---|---|---|
| Negative | A+A Band | Normal |
| Positive | A+S Band | Carrier |
| Positive | S+S Band | Sufferer |
Maharashtra Arogya Mandal is Non Profit Non-Government Organisation (NGO) :
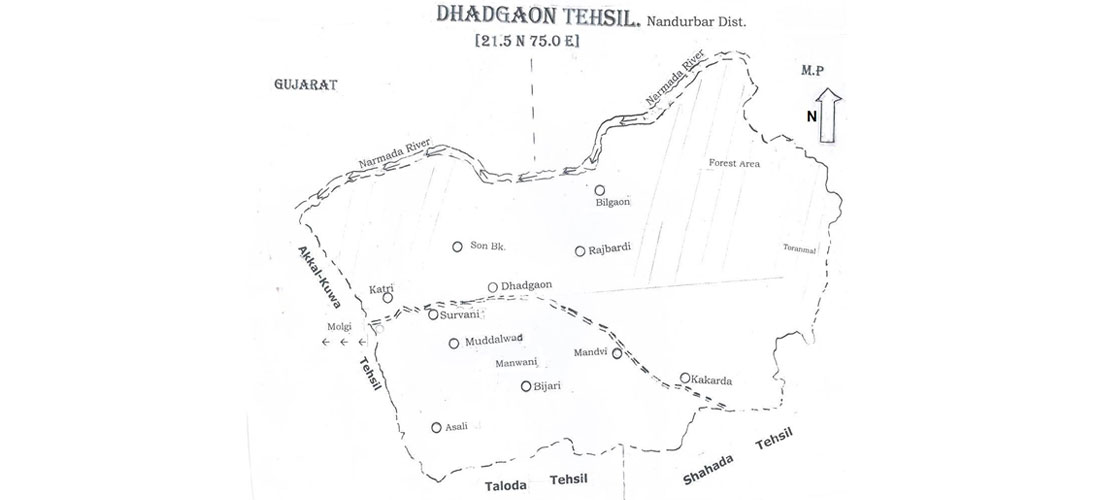
- Established at Hadapsar, Pune city, Maharashtra in 1960. It has several activities in field of health,education and tribal welfare. The institute has developed two centres in tribal areas, one known as Bhimashaknar tribal development centre at post Dimba, Tehsil Ambegaon, Dist. Pune and this centre involved in natural research management and water shed management for the tribal communities from this area. Another centre developed in Nandurbar dist. of Maharashtra. The centre is located in Hilly areas of Satpuda ranges at Roshmal BK. Tehsil Dhadgaon, Nandurbar district (21.5N - 75.0E) with mandate to provide diagnosis, treatment, counselling and prevalence for Sickle Cell Anaemia disease patients in this area.
Rationale: behind selecting Dhadgaon district for our work on Sickle Cell Anaemia:
- Dhadgaon Tehsil of Nandurbar Dist. is isolated from rest of the Maharashtra. This is geographically difficult hilly terrain of Satpuda ranges with total population of 98,000 (as per 1991 census). 96% population belongs to two tribal groups Bhill and Pawara. Transport facilities were poor and people from this area remain backward in all aspect of life i.e health and education.
- Dhadgaon Tehsil has total 163 villages. Initially we conducted population genetic survey for sickle cell disorder in 12 selected villages and found out that sickle cell anaemia to be major health problem in tribal communities. The prevalence for carrier is of 22.5% and sufferer 1.25%.Government services for Sickle Cell patients are inadequate considering vast extent of the disease. Taking into consideration all above mentioned facts, we decided to work in this Tehsil and established community control programme centre popularly known as Sickle Cell Dawakhana.This is a community health service centre with support of locals.
| Sr No | Tribe/Scheduled caste | Total screened | A+A Normal | A+S Carrier | S+S Sufferer |
|---|---|---|---|---|---|
| 1 | Bhill (Tribe) | 4184 | 3253 | 871 | 60 |
| 2 | Pawara (Tribe) | 701 | 504 | 183 | 14 |
| 3 | Scheduled caste | 97 | 82 | 13 | 2 |
| Total | 4982 | 3839 | 1067 | 76 | |
| 77.05% | 21.47% | 152% |
- Initially in 1998 we used to visit major villages from different part of this tehsil with mobile unit and carry out our activities of diagnosis, treatment counselling and prevention. Our initial work in this part was not easy. We have to face several difficulties regarding accommodation, food, permanent space for laboratory, electrical supply, transport and many others. In 2004, we have our own building in this area and were easy to plan our work more systematically.
Information of our activities is as follows: :
- We organised our major health camps, at the interval of two months, where facilities for diagnosis, ayurvedic treatment counselling and prevention are made available. In addition to this doctor and laboratory technicians are available on every Monday and Tuesday for patient service
- We have developed herbal medicine in our pharmacy, the drug is known as SC3 and very effective in controlling severe symptoms of the disease. Patients are happy with our herbal medicine.
- Patients attending our clinics are divided in two groups, one who are diagnosed previously at our centre and come for medical check-up, drug and counselling. We discuss with every patients about illness during last two months, suggest any changes in medicine, further instructions for diet and what to do and not to do for keeping good health. Every patient received drug for next two months. We write down all his findings in a note book given to them and also keep record in our file. We instruct patient, that for any acute illness in between next two months, she/he should approach nearest medical officer along with note book so that treating physician gets information about diagnosis treatment given and follow up.
- Another group of individuals attending our clinic are new comers having symptoms of Sickle Cell Anaemia. We prepare their case paper, write down all details on their case paper regarding full name, age/sex; details about their address. After that their blood is collected for diagnosis and when Sickle Cell Status is known they are divided in three groups, one Sickle Cell Anaemia patient, another carrier, and third Normal (without Sickle Cell Defect).
- We provide identity cards Red to sufferer, Yellow to Carrier and White to normal individuals. Details examination of every new diagnosed patient carried out and discuss with them about various aspects of the disease, drug information and instruction for follow up. We suggest every patient for his/her family members to check up for Sickle Cell Status and ask them to bring them for next visit. We write in their note book, dates about next major camp
- To a carrier and normal individuals, we explain about counselling, particularly marriage counselling to avoid further birth of sickle cell child. We provide pamphlet written in a local language in which all information about disease drug available and different counselling procedures. We insist on that their family members to be checked for sickle cell status
- We keep details record of all patients attending our clinic. We have now 2492 patients suffering from Sickle Cell Anaemia under our medical treatment.
Our Work Details :
- Sickle Cell Dawakhana centre started in 1998 in Dhadgaon Tehsil (Nandurbar Dist.) with mandate to provide diagnosis, treatment, counselling and preventive facilities to tribal population from this tehsil.
- We have screened about one lakh tribal individuals from Nandurbar Dist. For Sickle Cell disorder and found 22.2% heterozygotes and 1.25% Homozygotes (Sufferer)
- We have now more than 2500 patient under our medical supervision. We formulated our own ayurvedic drug known as SC3, which we find it very useful for controlling severe symptoms of Sickle Cell disease. Central council for research in Ayurveda and Siddha, Dept. of AYUSH, Ministry of Health and Family welfare New Delhi has sanctioned funds to take trial of this drug. During this trial we have carried out Haematological and Biochemical marker studies of Sickle Cell Patient. On the basis of this central government AYUSH Dept. has approved our drug. Our patients are happy with the drug.
- Ours being voluntary health organisation (NGO), We Provides diagnosis, treatment, counselling and Preventive facilities free of cost.
- The disease pattern of our patients, as compare with patients from Africa is milder type. Our patients have longer life span. However we found that all reported complications of the disease except priapism and leg ulcers in our patients
- We have carried out ultra sonographic studies of abdomen of 204 patient and found splenomegaly of various sizes in 114 patients (55%).
- We carried out ophthalmic check-up for retinopathy of 105 Sickle Cell patients. Five patients have suspected retinopathy. These patients needs follow up.
- The land on which our Sickle Cell Dawakhana building stands is donated by one of the tribal youth Mr. Manoj Pawra. All administration of the centre is carried by local tribal youth.
- Since 2013, every year we celebrate international Sickle Cell Day as declare by UNESCO. Every year we organise free blood testing camp and organise meeting of patients, parents, teachers, Social workers and people to create awareness among them
- In 2015 Maharashtra University of health sciences at Nashik awarded Lifetime achievement award 2015 to Head of our Sickle Cell Department- Dr. S. L. Kate. for his work on sickle cell anaemia among tribal people in Maharashtra.
- We have carried out haemoglobin estimation of all individuals visiting our clinic and found haemoglobin concentration (less than 10 gms) in Sickler and non Sickler individuals. Low haemoglobin suggest that proteins, vitamins and minerals require to synthesis in body are inadequate. Tribal people residing in this part have no other source of income except agricultural. The land here is not fertile and has limited income source Low haemoglobin is outcome of malnutrition. People from this area particularly ladies and children are in need of good supplementary diet.
- On this nutritional insufficient back group we prepare approximately 300 nutrition Laddu in our pharmacy. Corn (Maka) is chief source of diet available in this part. Corn is lacking essential amino acid lysine. Good source of lysine is Amaranth. We have done R & D tests of these two products and prepare a mixture of these products, so that first class proteins are available to them. In additional to this we add easily available seeds of Kernel of Muskmelon (Magaj Bee) and other mineral Supply and prepare Nutritional Laddu. We prepare dietary note on this and suggest all mothers visiting our clinic along with patients that all ingredient require for this nutritious food are available in local market and encourage mothers to prepare on their own.
Impact of our work:
- By our sincere efforts we are able to create awareness among the people for sickle cell disease without any advertisement of our work. Patients even from long distance (Madhya Pradesh and Gujarat state) visit our centre to know the Sickle Cell Status. Increase in number of patients at every bi-monthly camp is indication of this effect.
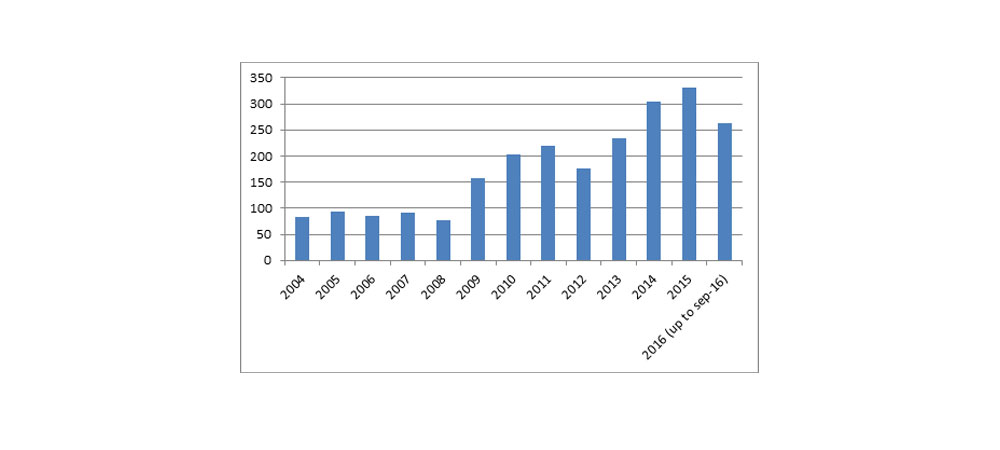
- Since 2004, when we have our own building, we are able to organise our work systematically. Following year wise data indicate our progress.
Sickle Cell Patients identified from Last 12 years
| Year | No. of Sickle Cell Patients identified |
|---|---|
| 2004 | 83 |
| 2005 | 94 |
| 2006 | 85 |
| 2007 | 91 |
| 2008 | 78 |
| 2009 | 158 |
| 2010 | 203 |
| 2011 | 220 |
| 2012 | 117 |
| 2013 | 233 |
| 2014 | 304 |
| 2015 | 330 |
| 2016 (up to sep-16) | 263 |
Graph of No. of Sickle Cell Patients identified from last 12 years
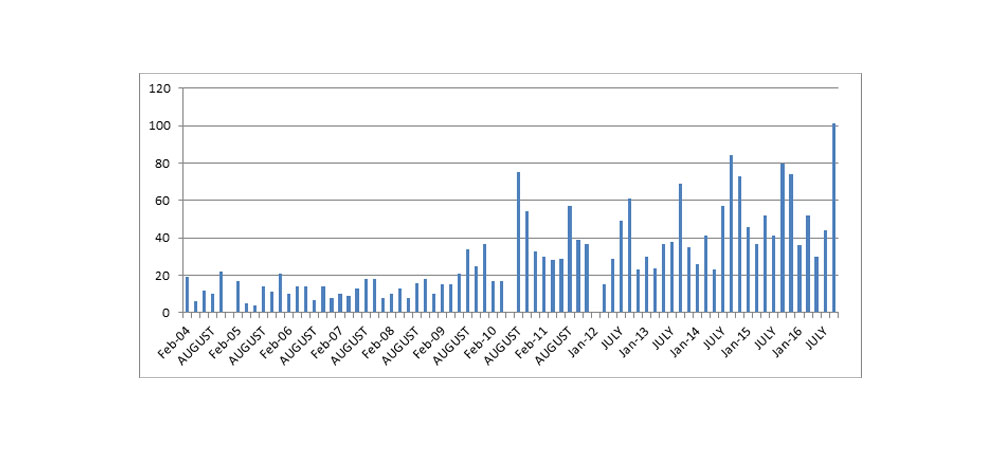
TOTAL NUMBER OF NEW PATIENTS- Month and year wise (from 2004 to 2016) at DHADGAON
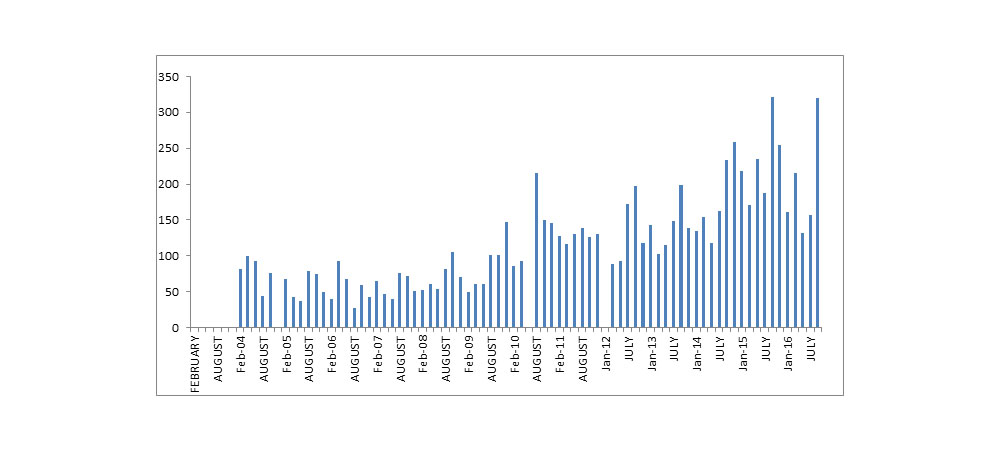
TOTAL NUMBER OF SS PATIENTS- Month and year wise (from 2004 to 2016) at DHADGAON
Our future Activities:
- Our aim is to avoid birth of sickle cell child and we are making sincere efforts for our motto. We will provide prenatal diagnosis facilities to all couples who have this defect to avoid birth of sickle cell child. We are planning to have full-fledged hospital in which all medical facilities are available to all Sickle Cell patients free of cost.
- Pusanwahan sanskar is one of the methods to have healthy baby had been described in ayurvedic text. We will try to introduce this concept to sickle cell carrier couples.
- Dr. Frederic B. Piel, a well-known world scientist in the field of statistics and demography postulated in his publication (PLOS medicine July 2013/ volume 3/ issue 7 e 100148/ page no 1 to 14) that if proper prevention and management to sickle cell patient is not made available than by 2050 India including some African country will be capital for Sickle Cell Anaemia disease. Taking into consideration gravity of the problem, our centre is implementing strategies to provide all facilities to Sickle Cell patients.